Adrenal Tumors – Types, Diagnosis & Questions
So this topic is about adrenal tumors and some of the really common questions that they actually test on step 1 and Nclex. So before anything starts off on, just the basics of physiology, what we have here is the pituitary gland and what the pituitary gland does is that it releases hormones, one of the hormones it releases is ACTH.
WATCH VIDEO ONE OF THE BEST LECTURE ON ADRENAL TUMORS
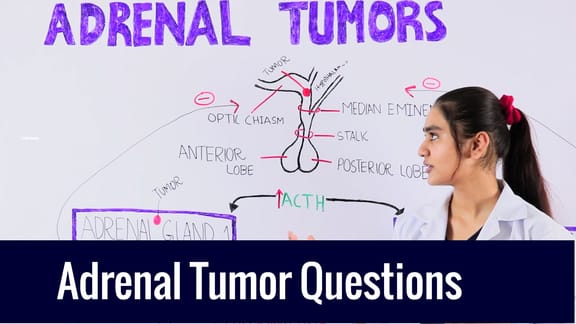
Physiology of Pituitary Gland
Now, what does ACTH do? It goes to both of your adrenal glands, adrenal gland one and adrenal gland 2. And once it goes to the adrenal gland what does it do? It helps actually stimulate the release of cortisol and aldosterone on both sides. Now, not only does it stimulate the release of hormones, it actually causes the growth of cells, especially the cells and the glands here. This, basically endocrine gland requires ACTH to remain alive and to grow. Okay, so there are two things that ACTH is doing,
- It is actually inhibiting apoptosis, and
- Actually causing the gland to grow more or to proliferate and to stay alive.
Adrenal Tumor
Now, what happens if I have a pituitary tumor? Now, what happens if I have a pituitary tumor here?
1st scenario, a tumor that’s releasing a lot of ACTH, so I have a lot of ACTH coming through, what is it gonna do? It’s gonna go to both adrenal glands and it will cause a growth of these glands, because it is making sure these cells stay alive and that they are growing at the same time. So, we have a lot of ACTH, stimulates both of these glands, and what does it do? A lot of cortisol and a lot of aldosterones. So what are we gonna see? What does aldosterone do? Reabsorbs sodium gets rid of potassium, and it helps to reabsorb bi-carbs also. So, with high aldosterone levels we see, hypernatremia, hypokalemia, and alkalosis. These are the three things really common electrolyte abnormalities and they love to ask questions, where initially in the question they’ll give you lab values and they’ll show you sodium is really high, the potassium is really low and they’ll say oh the PH was let’s say 7.6 or 7 6, and they’ll ask you to connects the dots. So we have a pituitary tumor, high ACTH, cortisol, aldosterone, etc. If with cortisol it’s known as Cushing syndrome and with aldosterone, it’s known as conn’s syndrome right where it’s high aldosteronism.
Pathophysiology of Adrenal Tumors
Now the second point I wanted to make here is when this cortisol and aldosterone gets released, what does it do? It goes back and actually inhibits the release of ACTH, this cortisol and aldosterone are going back and saying to the pituitary gland, STOP RELEASING ACTH! Let’s say, for example, the pituitary tumor is gone now, we have a normal person and now they have a tumor in adrenal gland 1, and what is this tumor releasing, it’s releasing a lot of cortisol, it’s release aldosterone, one of the two, it doesn’t matter right now. So it releases a ton of it, a ton of it!
Well, if it’s releasing a lot of aldosterone and cortisol, what’s the other side releasing? Well saying, you know adrenal gland number 1 is doing way much more of a job than the body needs, and two is just laying back and not doing anything, I mean not releasing much of hormones. This cortisol and aldosterone goes back and inhibits ACTH, Now what do we say ACTH is required to do? The glands need ACTH to remain alive and to grow. So we don’t have to come out of the pituitary anymore and it’s not stimulating the glands and as a result, there’s no more ACTH. But this tumor that’s here does not need ACTH to stay alive and to grow, whereas this gland number, adrenal gland number 2 needs ACTH to stay alive, so what happens?
After a long time of having this tumor released a lot of cortisol and aldosterone, your body spends a lot of time without ACTH and if it spends a lot of time without ACTH, what’s gonna happen to the cell? This adrenal gland here, this endocrine gland will no longer remain alive and it won’t grow, so it shrinks. It becomes smaller and smaller and it basically atrophies. So I have a patient who has really high cortisol and aldosterone because of this tumor, and its other gland is basically gone, it’s shot! There’s nothing of it. So what happens after I do surgery to remove this adrenal tumor? So if I take it out, what happens to my cortisol levels will drop, I’ll drop my aldosterone levels also but now your body says I don’t have new cortisol and aldosterone because your pituitary spends so much time without releasing ACTH that this factory shuts down.
So now your body can’t respond to any stress and create any cortisol and aldosterone. That’s why the patients adrenal-ectomies and their other adrenal gland is completely shot, they go into basically a cardiovascular collapse. They become hypertensive etc because they don’t have any more cortisol, and aldosterone because the one gland that was working they actually had was taken out.
So what other types of questions can they ask you? They love asking this one question where they say, they give you a scenario, a patient has a tumor, they have high sodium, low potassium, basically make you wanna think hyper-aldosteronism. And they say it’s from an adrenal tumor that’s releasing it. Then they say, we removed the tumor and we decided to do a CT scan, what would you expect to see on the CT scan? An atrophic adrenal gland! The other one that does not have the tumor will be atrophied and they love asking that question. So just by that simple you know thing, you test a lot of different concepts. You test anatomy, you test physiology, with this whole negative feedback. They want to see if you know how this entire mechanism works, how ACTH is released, how cortisol is released, and how negative feedback works.
Okay, so that was about the adrenal tumors. Thank you so much for reading this article and please consider subscribing to my YouTube channel. Also, don’t forget to check out my website to watch one of the best videos that are part of this series as well.